What Is the BCT Taxonomy?
The BCT Taxonomy (Behaviour Change Technique Taxonomy version 1, or BCTTv1) is a standardized classification of 93 distinct behavior change techniques organized into 16 groupings. It provides a common language for describing, coding, and comparing the “active ingredients” of behavior change interventions. Developed by a multi-institutional team led by Susan Michie, including Michelle Richardson, Marie Johnston, Charles Abraham, Jill Francis, Wendy Hardeman, Martin Eccles, James Cane, and Caroline Wood, the taxonomy was published in 2013 in Annals of Behavioral Medicine.
The taxonomy answers a deceptively simple question: “What exactly did the intervention do?” Before BCTTv1, two researchers describing the “same” intervention might mean completely different things. One study’s “goal setting” might be another’s “action planning.” The taxonomy assigns each technique a precise definition, a numerical label (e.g., 1.1, 2.3), and clear criteria for distinguishing it from similar techniques.
The BCTTv1 paper has accumulated over 7,000 citations, making it one of the most cited papers in behavioral science. It sits within the broader Behaviour Change Wheel (BCW) system as the practical layer that translates intervention strategies into specific, replicable techniques.
How the Taxonomy Was Built
The BCT Taxonomy was not assembled casually. The development process spanned multiple years and followed a rigorous Delphi consensus method.
Step 1: Compilation. The research team compiled candidate techniques from existing published taxonomies, including Abraham and Michie’s earlier 26-technique taxonomy (2008, Health Psychology), the CALO-RE taxonomy (Michie et al., 2011), textbooks, and intervention manuals. This produced an initial list of 124 candidate techniques.
Step 2: Expert Delphi exercise. An international panel of behavior change experts participated in iterative rounds of rating and refinement. Experts rated each technique for clarity, distinctiveness, and whether it belonged in the taxonomy.
Step 3: Sorting and clustering. Experts independently sorted the techniques into groups. Hierarchical cluster analysis identified 16 natural groupings.
Step 4: Reliability testing. Trained coders independently coded intervention descriptions to test whether they could reliably identify the same techniques. Inter-rater reliability was assessed and reported.
The result: 93 techniques survived the process. Each received a standardized name, a numerical label, a precise definition with examples, and clear boundary criteria.
The 16 Groupings
1. Goals and Planning
The most frequently used grouping in intervention design. Includes goal setting for behavior (1.1), problem solving (1.2), goal setting for outcomes (1.3), action planning (1.4), and behavioral contract (1.8). Action planning (1.4) is essentially the formal name for implementation intentions (“if X happens, I will do Y”).
2. Feedback and Monitoring
Includes self-monitoring of behavior (2.3) and feedback on behavior (2.2). Self-monitoring is the single most consistently effective BCT across meta-analyses. Michie and colleagues (2009) found that interventions including self-monitoring produced significantly larger effects (d = 0.42) than those without it (d = 0.26) when combined with at least one other self-regulation technique.
3. Social Support
Three variants: unspecified (3.1), practical (3.2), and emotional (3.3). Advise on, arrange, or provide social support for the target behavior.
4. Shaping Knowledge
Includes instruction on how to perform the behavior (4.1) and information about antecedents (4.2). These address the “I don’t know how” barrier.
5. Natural Consequences
Includes information about health consequences (5.1), salience of consequences (5.2), and anticipated regret (5.5). These techniques make the costs and benefits of the behavior psychologically vivid.
6. Comparison of Behavior
Includes demonstration of the behavior (6.1, modeling), social comparison (6.2), and information about others’ approval (6.3). Social comparison draws on normative influence. Demonstration draws on Bandura’s observational learning.
7. Associations
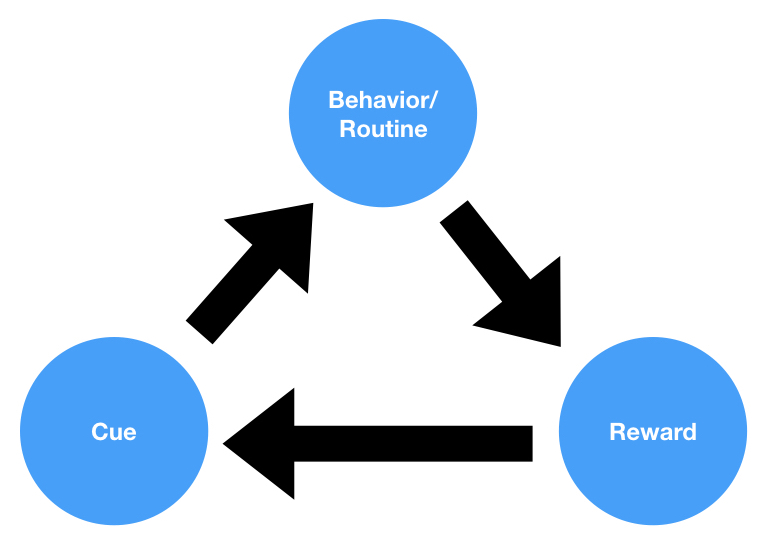
Includes prompts/cues (7.1), the technique of introducing environmental or social stimuli to trigger the behavior. Also includes cue signaling reward (7.2) and associative learning (7.8).
8. Repetition and Substitution
Includes behavioral practice/rehearsal (8.1), behavior substitution (8.2), habit formation (8.3), and graded tasks (8.7). Habit formation (8.3) specifically prompts rehearsal and repetition in the same context to build automaticity.
9. Comparison of Outcomes
Includes credible source (9.1) and pros and cons (9.2). These help people evaluate reasons for and against changing their behavior.
10. Reward and Threat
The largest grouping with 11 techniques, covering material incentives (10.1), material rewards (10.2), social rewards (10.4), and self-rewards (10.9). The taxonomy carefully distinguishes between incentives (promises of future reward) and rewards (delivered after the behavior).
11. Regulation
Includes pharmacological support (11.1) and conserving mental resources (11.3). These address physiological and cognitive barriers.
12. Antecedents
Includes restructuring the physical environment (12.1) and restructuring the social environment (12.2). These overlap conceptually with choice architecture. Also includes adding objects to the environment (12.5), which during COVID-19 covered placing hand sanitizer stations and providing free masks.
13. Identity
Includes framing/reframing (13.2) and valued self-identity (13.4). James Clear’s “identity-based habits” concept maps directly to this grouping.
14. Scheduled Consequences
Operant conditioning techniques: behavior cost (14.1), punishment (14.2), remove reward (14.3), and various reinforcement schedules.
15. Self-Belief
Includes verbal persuasion about capability (15.1) and focus on past success (15.3). These target self-efficacy, the construct Albert Bandura identified as the strongest cognitive predictor of behavior change.
16. Covert Learning
Includes imaginary punishment (16.1), imaginary reward (16.2), and vicarious consequences (16.3). Mental rehearsal techniques drawn from cognitive behavioral therapy.
How BCTs Connect to COM-B and the Behaviour Change Wheel
The BCT Taxonomy is the innermost practical layer of a three-part system:
Layer 1: COM-B (diagnosis). Identifies why the behavior is not happening. Is the barrier Capability, Opportunity, or Motivation?
Layer 2: Intervention Functions (strategy). The BCW’s nine intervention functions (Education, Training, Enablement, Persuasion, Incentivisation, Coercion, Environmental Restructuring, Modelling, Restriction) translate the COM-B diagnosis into a type of intervention.
Layer 3: BCT Taxonomy (specific techniques). Each intervention function maps to multiple BCTs. For example, the “Training” function maps to behavioral practice/rehearsal (8.1) and graded tasks (8.7). The “Environmental restructuring” function maps to restructuring the physical environment (12.1) and prompts/cues (7.1).
The Theory and Techniques Tool (Connell et al., 2019, Annals of Behavioral Medicine) extends this further by mapping 74 BCTs to 26 mechanisms of action. For example, goal setting (1.1) works through mechanisms of intentions, goals, and behavioral regulation. Self-monitoring (2.3) works through behavioral regulation and beliefs about capabilities. This creates a formal chain: COM-B diagnosis, to intervention function, to BCT, to mechanism of action.
Which BCTs Work Best? The Meta-Analytic Evidence
No single BCT works universally. But meta-analyses consistently identify a small cluster of techniques that outperform others across multiple behavioral domains.
Self-monitoring (2.3) combined with goal setting (1.1) is the most reliably effective combination. Michie and colleagues (2009) found this pair across physical activity and dietary interventions. Subsequent reviews confirmed it for weight management, diabetes self-management, and medication adherence.
Self-monitoring alone is the single most effective individual BCT. Dombrowski and colleagues (2012) confirmed this in a meta-analysis of weight loss interventions for obese adults with comorbidities.
Action planning (1.4) draws on the implementation intentions literature. Gollwitzer and Sheeran’s 2006 meta-analysis found a medium-to-large effect size (d = 0.65) across 94 studies for implementation intentions.
Prompts/cues (7.1) and environmental restructuring (12.1) were among the most effective techniques for COVID-19 pandemic behaviors. Hand sanitizer stations, floor markings for distancing, one-way systems in stores, and mask provision all map to these BCTs.
Webb and colleagues (2010) found that internet-based health behavior change interventions grounded in theory (which facilitated systematic BCT selection) produced larger effects (d = 0.50) than atheoretical interventions (d = 0.33).
Carey and colleagues (2019) mapped links between 56 BCTs and their mechanisms of action, synthesizing evidence from published intervention literature to identify which techniques work through which psychological pathways.
Real-World Applications
COVID-19 Pandemic Response
The BCT Taxonomy became a critical tool for coding and designing pandemic interventions. West and colleagues (2020) published analyses coding public health messaging using BCT labels. Arden and colleagues (2021) applied the taxonomy to self-isolation adherence in the British Journal of Health Psychology. Denford and colleagues (2021) used BCT coding to evaluate COVID-19 public health communications and found inconsistent use of techniques across government messaging.
NHS Stop Smoking Services
West and colleagues (2010) used BCT coding to analyze England’s Stop Smoking Services. The most effective combination included pharmacological support (11.1), self-monitoring (2.3), advice on quitting methods, and social support. Four-week quit rates reached approximately 35%, compared to 3-5% for unassisted quit attempts.
Physical Activity and Diet
Michie and colleagues (2009) conducted a meta-regression of 122 interventions for physical activity and healthy eating. Interventions combining self-monitoring with at least one other technique from control theory (goal setting, feedback on performance, review of behavioral goals) produced significantly larger effects than those without this combination.
Limitations and Criticisms
93 techniques is unwieldy for practitioners. Most clinicians, public health workers, and product designers cannot memorize or navigate the full taxonomy. Training to reliably code BCTs takes approximately 6-10 hours through the online course, with ongoing practice needed to maintain reliability.
The taxonomy tells you WHAT, not WHICH. Knowing that 93 techniques exist does not tell a practitioner which to select for a given problem. The COM-B/BCW framework partially addresses this gap, but the mapping from COM-B components to specific BCTs still involves considerable judgment. There is no algorithm that says “for this specific barrier, use these specific BCTs.”
Same BCT, vastly different delivery. “Goal setting (behavior)” could be a collaborative conversation with a coach, a form on a website, a text message prompt, or a group exercise. These different delivery modes likely produce different effects, but the taxonomy treats them identically. Mode, dose, timing, and tailoring are all critical but not captured.
Reliability varies across groupings. Even with training, some BCTs are harder to identify reliably than others. Techniques in Groups 13 (Identity), 16 (Covert Learning), and 14 (Scheduled Consequences) tend to have lower inter-rater reliability scores. The distinction between some BCTs is subtle (“information about health consequences” versus “salience of consequences” versus “anticipated regret”).
Cultural generalizability. The taxonomy was developed primarily by UK and European researchers. Social comparison (6.2) may function differently in collectivist versus individualist cultures. Self-monitoring (2.3) assumes literacy and access to recording tools. Identity-based techniques (Group 13) may interact with cultural conceptions of self.
BCT Taxonomy vs. Other Frameworks
| Feature | BCT Taxonomy | COM-B / BCW | EAST | Fogg (B=MAP) |
|---|---|---|---|---|
| Purpose | Specify intervention content | Diagnose behavior, select intervention type | Practitioner checklist | Product design heuristic |
| Granularity | 93 techniques in 16 groupings | 6 subcomponents, 9 intervention functions | 4 principles | 3 factors |
| Audience | Researchers, intervention designers | Health researchers, policymakers | Frontline practitioners | Product designers |
| Strength | Precision, replicability, cumulative science | Comprehensive diagnosis | Memorable, fast | Intuitive, actionable |
| Weakness | Overwhelming for non-specialists | Complex, requires training | Oversimplifies | Near-zero formal validation |
In practice, the most effective teams use these frameworks together. COM-B diagnoses the behavioral barrier. The BCW selects the intervention function. The BCT Taxonomy specifies the exact techniques. EAST or MINDSPACE provides a quick design check.
Frequently Asked Questions
What is the BCT Taxonomy? The BCT Taxonomy (BCTTv1) is a standardized classification of 93 behavior change techniques organized into 16 groupings. Each technique has a precise definition, a numerical label, and examples. It was developed by Susan Michie and colleagues at UCL and published in 2013. The taxonomy provides a common language for describing, coding, and comparing the “active ingredients” of interventions.
What are the most effective behavior change techniques? Meta-analyses consistently identify self-monitoring of behavior (BCT 2.3) as the single most effective individual technique. When combined with goal setting (BCT 1.1), the pair produces significantly larger effects than either alone. Action planning (BCT 1.4, based on implementation intentions) also shows strong effects across domains, with a meta-analytic effect size of d = 0.65.
How does the BCT Taxonomy relate to COM-B? The BCT Taxonomy is the practical technique-selection layer within the broader Behaviour Change Wheel system. COM-B diagnoses why a behavior is not occurring (Capability, Opportunity, or Motivation deficit). The BCW maps that diagnosis to nine intervention functions. The BCT Taxonomy then specifies which of the 93 techniques deliver each intervention function.
How do you use the BCT Taxonomy? For intervention design: start with a COM-B behavioral diagnosis, select intervention functions from the BCW, then use the BCT Taxonomy to choose specific techniques. For research: use the taxonomy to code existing interventions by reading descriptions and systematically identifying each BCT present using the standardized definitions. Training is available through a free online course at bct-taxonomy.com.
Is there a BCT Taxonomy version 2? As of early 2026, BCTTv2 has not been formally published as a complete updated taxonomy. The Human Behaviour-Change Project at UCL, led by Michie and colleagues with Wellcome Trust funding, has been developing a more comprehensive BCT Ontology using AI and machine learning. Individual refinements have been made to some technique definitions, and the Theory and Techniques Tool represents an evolution of the framework.
Sources and Further Reading
- Michie, S., Richardson, M., Johnston, M., et al. (2013). The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques. Annals of Behavioral Medicine, 46(1), 81-95.
- Abraham, C., & Michie, S. (2008). A taxonomy of behavior change techniques used in interventions. Health Psychology, 27(3), 379-387.
- Connell, L. E., Carey, R. N., de Bruin, M., et al. (2019). Links between behavior change techniques and mechanisms of action. Annals of Behavioral Medicine, 53(8), 708-720.
- Michie, S., Abraham, C., Whittington, C., McAteer, J., & Gupta, S. (2009). Effective techniques in healthy eating and physical activity interventions. Health Psychology, 28(6), 690-701.
- Gollwitzer, P. M., & Sheeran, P. (2006). Implementation intentions and goal achievement: A meta-analysis. Advances in Experimental Social Psychology, 38, 69-119.
- Webb, T. L., Joseph, J., Yardley, L., & Michie, S. (2010). Using the internet to promote health behavior change. Journal of Medical Internet Research, 12(1), e4.
- Carey, R. N., et al. (2019). Behavior change techniques and their mechanisms of action. Annals of Behavioral Medicine, 53(8), 693-707.
- Dombrowski, S. U., et al. (2012). Identifying active ingredients in complex behavioural interventions for obese adults with obesity-related co-morbidities. Health Psychology Review, 6(1), 7-32.
- West, R., Walia, A., Hyder, N., Shahab, L., & Michie, S. (2010). Behavior change techniques used by the English Stop Smoking Services and their associations with short-term quit outcomes. Nicotine & Tobacco Research, 12(7), 742-747.
- West, R., et al. (2020). Applying principles of behaviour change to reduce SARS-CoV-2 transmission. Nature Human Behaviour, 4, 451-459.
- Arden, M. A., et al. (2021). Behavioural insights for self-isolating. British Journal of Health Psychology, 26(2), 267-283.
- Denford, S., et al. (2021). Understanding patterns of adherence to COVID-19 mitigation measures. Journal of Health Psychology, 26(13), 2530-2542.