What Is the COM-B Model?
The COM-B model is a behavioral science framework stating that three conditions must be present for any behavior to occur: Capability (C), Opportunity (O), and Motivation (M), which together produce Behavior (B). Developed by Susan Michie, Maartje van Stralen, and Robert West at University College London, COM-B was published in 2011 in Implementation Science and has since become the most widely cited behavior change model in the world, with over 15,000 academic citations.
COM-B is a diagnostic model. It answers the question: “Why isn’t the behavior happening?” Each of the three components breaks into two subcomponents, creating six possible reasons a behavior might fail. This makes COM-B systematically useful in ways that simpler frameworks (like EAST or the Fogg Behavior Model) are not.
COM-B sits at the center of the Behaviour Change Wheel (BCW), a broader intervention design system that maps behavioral diagnosis to specific intervention strategies and policy options.
The Three Components (and Six Subcomponents)
Capability: Can They Do It?
Physical Capability covers the physical skills, strength, and stamina needed to perform the behavior. A person who cannot physically open a childproof medicine bottle lacks the physical capability for medication adherence. A person with limited mobility may lack the physical capability for a stair-climbing intervention.
Psychological Capability covers the knowledge, cognitive skills, and mental capacity required. A person who does not know what constitutes a “healthy portion size” lacks psychological capability for dietary change. Healthcare workers who cannot remember the correct hand hygiene protocol at the right moment have a psychological capability deficit.
Barker, Atkins, and de Lusignan (2016) demonstrated the COM-B diagnostic process in the International Journal of Audiology by applying it to hearing aid use in adult auditory rehabilitation. They found that psychological capability (understanding how to use and maintain hearing aids) and reflective motivation (beliefs about the value of hearing aids) were key barriers. The study illustrates COM-B’s strength: systematically identifying which of the six subcomponents is the bottleneck for a given behavior.
Opportunity: Does the Environment Allow It?
Physical Opportunity refers to what the external environment provides: time, resources, locations, physical access, and cues. No amount of motivation to exercise will help if the nearest gym is 30 miles away. A workplace with no recycling bins cannot expect recycling behavior.
Social Opportunity refers to cultural norms, social cues, and interpersonal influences. Whether colleagues smoke together during breaks. Whether a workplace culture normalizes overwork. Whether friends encourage or mock healthy eating attempts.
Motivation: Do They Want to Do It Enough?
Reflective Motivation covers conscious processes: planning, goal-setting, evaluating pros and cons, forming intentions, and identity beliefs (“I am a runner”). It includes self-efficacy (the belief that you can succeed) and outcome expectations (the belief that the behavior will produce the desired result).
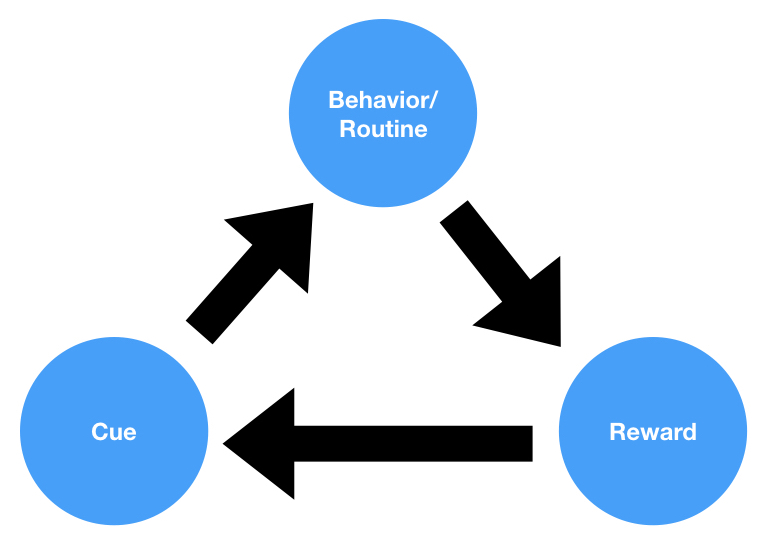
Automatic Motivation covers processes that happen without deliberate thought: emotional reactions, desires, impulses, and habits. The craving for a cigarette. The gut-level anxiety about a dental visit. The automatic habit of reaching for a phone when bored.
Qualitative studies using COM-B and the Theoretical Domains Framework have examined antibiotic prescribing among general practitioners and nurse prescribers (Courtenay et al., 2019, BMJ Open). These analyses consistently find that automatic motivation (the habitual pattern of prescribing “just in case” and the emotional discomfort of potentially leaving a patient untreated) is a primary driver of overprescribing, often outweighing knowledge deficits and guideline awareness.
How the Components Interact
COM-B is a dynamic system, not a static checklist. The components influence each other:
- Capability affects Motivation. Lacking the skill to do something erodes self-efficacy (reflective motivation drops) and creates frustration (automatic motivation drops). Building capability through practice builds confidence.
- Opportunity affects Motivation. If healthy food is unavailable (physical opportunity), intentions to eat healthily weaken (reflective motivation). If everyone around you smokes (social opportunity), the desire to quit fades (automatic motivation).
- Motivation drives Capability-seeking and Opportunity-seeking. A motivated person will seek training and restructure their environment. Without motivation, available capability and opportunity go unused.
- Behavior feeds back. Successfully performing a behavior changes future capability (skill improves), opportunity (new social connections), and motivation (confidence grows). The system is self-reinforcing.
The Behaviour Change Wheel
COM-B sits at the hub of a three-layer system:
Inner ring: COM-B (behavioral diagnosis, described above)
Middle ring: Nine Intervention Functions. These are categories of intervention that address COM-B deficits:
| Intervention Function | What It Does | COM-B Target |
|---|---|---|
| Education | Increases knowledge/understanding | Psychological Capability |
| Training | Imparts skills | Physical + Psychological Capability |
| Enablement | Reduces barriers beyond education/training | Capability + Opportunity |
| Persuasion | Uses communication to stimulate action | Reflective + Automatic Motivation |
| Incentivisation | Creates expectation of reward | Motivation |
| Coercion | Creates expectation of punishment | Motivation |
| Environmental Restructuring | Changes the physical/social context | Opportunity + Automatic Motivation |
| Modelling | Provides examples to imitate | Motivation + Social Opportunity |
| Restriction | Reduces opportunity for competing behaviors | Opportunity |
Outer ring: Seven Policy Categories that deliver the intervention functions: Communication/marketing, Guidelines, Fiscal measures, Regulation, Legislation, Environmental/social planning, and Service provision.
How to Use COM-B in Practice
Michie, Atkins, and West codified the process in their 2014 book The Behaviour Change Wheel: A Guide to Designing Interventions. Three stages:
Stage 1: Understand the Behavior
Step 1: Define the problem in behavioral terms. Not “people are unhealthy” but “adults aged 40-65 with type 2 diabetes are not performing 150 minutes of moderate-intensity physical activity per week.”
Step 2: Select the target behavior. List all behaviors that could address the problem. Score them on likely impact, likelihood of change, spillover effects, and measurability. Select 1-3 targets.
Step 3: Specify the behavior. Define who, what, when, where, how often, and with whom.
Step 4: Run the COM-B analysis. For each of the six subcomponents, assess: “Is this a barrier to the target behavior?” Use interviews, surveys, observation, or existing data.
The Theoretical Domains Framework (TDF) provides a more granular diagnostic within COM-B. Its 14 domains map onto the six COM-B components, offering finer-grained diagnosis for complex behaviors.
Stage 2: Identify Intervention Options
Map COM-B deficits to intervention functions. Filter options using the APEASE criteria: Affordability, Practicability, Effectiveness/cost-effectiveness, Acceptability, Side-effects/safety, and Equity.
Stage 3: Select Behavior Change Techniques
Use Michie and colleagues’ BCT Taxonomy v1 (93 techniques organized into 16 clusters) to select specific techniques that operationalize each intervention function. For example, if the intervention function is “Training” to address a physical capability deficit, specific BCTs might include “Demonstration of the behavior” (BCT 6.1) and “Behavioral practice/rehearsal” (BCT 8.1).
Real-World Applications
COVID-19 Pandemic Response
COM-B became the most widely used behavioral framework during the pandemic. The UK government’s Scientific Pandemic Influenza Group on Behaviours (SPI-B), of which Susan Michie was a prominent member, used COM-B to structure advice on mask-wearing, hand washing, social distancing, and vaccine uptake.
West and colleagues (2020) published “Applying principles of behaviour change to reduce SARS-CoV-2 transmission” in Nature Human Behaviour, using COM-B to categorize all pandemic-relevant behaviors and map them to intervention strategies. The paper has been cited over 1,000 times.
Sherman and colleagues (2021) used COM-B to analyze vaccine hesitancy among 1,500 UK adults, published in Human Vaccines & Immunotherapeutics. Reflective motivation (beliefs about vaccine safety) was the strongest predictor of vaccine intention. Social opportunity (perceiving that friends and family supported vaccination) was second.
Workplace Sitting Reduction
Edwardson and colleagues used COM-B to design the “Stand More AT Work” (SMArT Work) intervention. The cluster randomized controlled trial across NHS offices found the COM-B-designed intervention reduced sitting time by 50 minutes per 8-hour workday at 3 months and 83 minutes at 12 months (Edwardson et al., 2018, BMJ). Follow-up research indicated effects were maintained over the longer term.
Sepsis Treatment Compliance
Steinmo and colleagues (2015) applied COM-B to understand why healthcare professionals did not follow sepsis treatment guidelines, published in Implementation Science. Social opportunity (team norms around escalation) and automatic motivation (confidence under pressure) were the primary determinants. The resulting COM-B-informed training program improved sepsis bundle compliance from 24% to 42%.
Smoking Cessation
NHS Stop Smoking Services adopted a COM-B-informed approach. Self-reported four-week quit rates reached approximately 35-50% (depending on year and region), compared to roughly 3-5% for unassisted quit attempts. Long-term quit rates are substantially lower, as relapse is common beyond the four-week window.
Limitations and Criticisms
Complexity. The full BCW system (COM-B + TDF + 9 intervention functions + 93 BCTs + 7 policy categories) is unwieldy for non-specialists. Connell and colleagues (2019) surveyed 277 health psychology researchers and practitioners. While 72% had heard of COM-B, only 31% had used the full BCW process, with most citing complexity and time requirements as barriers.
Self-report dependency. COM-B analyses typically rely on interviews and questionnaires. This creates a fundamental problem for automatic motivation (by definition hard to self-report) and physical opportunity (people may not recognize environmental constraints). Sniehotta, Presseau, and Araújo-Soares (2014) raised a related concern about self-report dependency in their critique of the Theory of Planned Behavior in Health Psychology Review. The same methodological limitation applies to COM-B.
Cultural applicability. COM-B was developed in the UK by UK-based researchers. Fewer studies have validated it outside Western, Educated, Industrialized, Rich, and Democratic (WEIRD) populations. Social opportunity norms vary dramatically across cultures. However, COM-B has been applied in sub-Saharan Africa (Pell et al., 2016, on malaria prevention in Ghana) and Southeast Asia, with reasonable results.
The “unfalsifiable” critique. Ogden (2016) argued in Health Psychology Review that COM-B is so broad it risks being unfalsifiable. If every behavioral determinant can be categorized under C, O, or M, the model “explains” everything and predicts nothing specific. Michie and West responded that comprehensiveness is a feature, not a bug: narrower theories miss important determinants, and COM-B’s value is in structuring diagnosis rather than making predictions.
No prompt/trigger component. Unlike the Fogg Behavior Model (B=MAP), COM-B does not include a trigger or cue as a separate element. Environmental cues fall under Physical Opportunity, but they are not given the distinct emphasis that product designers and habit researchers consider essential.
COM-B vs. Other Frameworks
| Framework | Diagnostic Power | Intervention Guidance | Ease of Use | Best For |
|---|---|---|---|---|
| COM-B / BCW | Highest (6 subcomponents + TDF) | Highest (9 functions + 93 BCTs) | Low (complex) | Health interventions, policy design, research |
| MINDSPACE | Moderate (9 influence channels) | Moderate (checklist) | Moderate | Policy practitioners, behavioral audits |
| EAST | Low (4 principles) | Moderate (actionable checklist) | High (memorable) | Frontline practitioners, quick design |
| Fogg (B=MAP) | Moderate (3 factors) | Low (general principles) | High (intuitive) | Product design, habit formation |
| Theory of Planned Behavior | Moderate (3 factors) | Low | Moderate | Research, predicting intentions |
COM-B and the Fogg Behavior Model share surface similarity (both identify motivation and capability/ability as key factors) but differ fundamentally. COM-B distinguishes reflective from automatic motivation and includes social/physical opportunity as explicit components. Fogg’s “Ability” conflates what COM-B separates into Capability and Physical Opportunity. COM-B provides a systematic pathway from diagnosis to intervention selection. Fogg provides design principles.
Frequently Asked Questions
What does COM-B stand for? COM-B stands for Capability, Opportunity, Motivation, and Behavior. The model states that all three factors (Capability, Opportunity, and Motivation) must be sufficiently present for a behavior to occur.
Who created the COM-B model? Susan Michie, Maartje van Stralen, and Robert West at University College London. The model was published in 2011 in Implementation Science. Michie later expanded the system with Lou Atkins and West in the 2014 book The Behaviour Change Wheel.
What is the difference between COM-B and the Behaviour Change Wheel? COM-B is the diagnostic core of the Behaviour Change Wheel (BCW). COM-B identifies why a behavior is or isn’t occurring. The BCW adds two outer layers: nine intervention functions (what type of intervention to use) and seven policy categories (how to deliver the intervention). COM-B diagnoses. The BCW prescribes.
How is COM-B different from the Fogg Behavior Model? Both models identify motivation and capability/ability as key factors. The differences: COM-B distinguishes between reflective motivation (conscious goals) and automatic motivation (habits, emotions). COM-B includes Opportunity (environmental and social factors) as a separate component. Fogg includes a Prompt/Trigger as a distinct element that COM-B does not. COM-B links to a systematic intervention design process (the BCW and BCT Taxonomy). Fogg provides design heuristics.
How do I use COM-B in practice? Define the target behavior precisely. For each of the six COM-B subcomponents (physical capability, psychological capability, physical opportunity, social opportunity, reflective motivation, automatic motivation), assess whether it is a barrier. Then use the Behaviour Change Wheel to map identified barriers to appropriate intervention functions, filtered by the APEASE criteria (Affordability, Practicability, Effectiveness, Acceptability, Side-effects, Equity).
Sources and Further Reading
- Michie, S., van Stralen, M. M., & West, R. (2011). The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implementation Science, 6, 42.
- Michie, S., Atkins, L., & West, R. (2014). The Behaviour Change Wheel: A Guide to Designing Interventions. Silverback Publishing.
- West, R., Michie, S., et al. (2020). Applying principles of behaviour change to reduce SARS-CoV-2 transmission. Nature Human Behaviour, 4, 451-459.
- Atkins, L., et al. (2017). A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implementation Science, 12, 77.
- Barker, F., Atkins, L., & de Lusignan, S. (2016). Applying the COM-B behaviour model and behaviour change wheel to develop an intervention to improve hearing aid use in adult auditory rehabilitation. International Journal of Audiology, 55(sup3), S90-S98.
- Sherman, S. M., et al. (2021). COVID-19 vaccination intention in the UK: Results from the COVID-19 vaccination acceptability study (CoVAccS). Human Vaccines & Immunotherapeutics, 17(6), 1612-1621.
- Edwardson, C. L., et al. (2018). Effectiveness of the Stand More AT (SMArT) Work intervention. BMJ, 363, k3870.
- Steinmo, S., et al. (2015). Characterising an implementation intervention in terms of behaviour change techniques and theory. Implementation Science, 10, 111.
- Ogden, J. (2016). Celebrating variability and a call to limit systematisation. Health Psychology Review, 10(3), 245-250.
- Connell, L. E., et al. (2019). Can surveys of health professionals inform the development of behaviour change interventions? Implementation Science, 14, 2.
- Sniehotta, F. F., Presseau, J., & Araújo-Soares, V. (2014). Time to retire the theory of planned behaviour. Health Psychology Review, 8(1), 1-7.
- Courtenay, M., et al. (2019). Examining influences on antibiotic prescribing by nurse and pharmacist prescribers: a qualitative study using the Theoretical Domains Framework and COM-B. BMJ Open, 9, e029177.